
Digital interventions for healthy ageing and cognitive health in older adults: a systematic review of mixed method studies and meta-analysis | BMC Geriatrics

Study selection
The database search yielded 2,909 articles. After applying limiters and removing duplicates, 1,991 articles were screened for title and abstract, and 29 were included for full-text screening. The eligibility of one study [43] appeared to be dissent between the reviewers due to the lack of a specific participant group outcome. Hence, the corresponding author of the article was contacted for further information. The study was included during the selection process, and the disagreement was resolved by all authors reaching a consensus on the quality assessment of the study. Sixteen studies were excluded from the 29 full-text screening. Of the 16 studies excluded, two studies were excluded because one was the phase one result of a research protocol, and another was the primary outcome from the study’s secondary analysis. The phase one results of a research protocol have the same results published in the research article that had been included in the review. The primary study of the secondary analysis was excluded because it was not related to the intervention or evaluation of the intervention. Another two studies were excluded because participants’ mean age was below 55. The rest of the twelve studies were excluded because they were not related to intervention or evaluation of intervention research. The final 13 studies were included in this review. Figure 1 summarises the study selection process adhering to the PRISMA guideline.

Preferred Reporting Item for Systematic Reviews and Meta-Analyses (PRISMA) flow chart for literature search [30]
Study characteristics and quality
Table 1 summarises the included study characteristics. Of thirteen studies included in this review (ntotal=19,551participants). Seven studies were quantitative research [6, 13, 17, 19, 22, 35, 43] (n=19,245 participants). Four studies were qualitative research, [3, 4, 18, 33] (n=260 participants). Two studies were mixed methods research [27, 42] (n=73 participants). Participants’ mean age ranged between 58 and 80 years. Three studies [3, 22, 43] (n=177) included both cognitively intact participants and participants with mild cognitive impairment, dementia, and cognitive decline. Only three studies specifically focused on improving the cognitive health of older adults [19, 22, 43] (n=13,651 participants), whereas two study interventions [17, 35] (n=2,871 participants) aimed to improve healthy ageing and cognitive health. For the meta-analysis of quantitative data, four quantitative studies presented dichotomous data [13, 19, 35, 43] and three quantitative studies presented continuous data [6, 17, 22].
The study appraisal using the MMAT is detailed in Table 1. Study quality assessments from the MMAT scores were between 3 and 5 indicating moderate to high study quality, with a low to moderate risk of bias. Table 2 shows the level of evidence matrix with MMAT score. The evidence matrix of each included study falls between levels 2 and 3, indicating a moderate to high level of study evidence [41].
All studies used digital technology to facilitate healthy ageing or maintain the cognition of older adults. Ten studies focused on healthy ageing in various health areas, including health literacy, self-health management, physical activity, social isolation, care dependency, health service communication, and assistive home living. Three studies focused on maintaining the cognitive health of older adults, including sustaining cognitive function by utilising technology to slow further cognitive decline or reduce the risk for dementia [19, 22, 43]. Two studies addressed their interventions for both healthy ageing and cognitive health of older adults [17, 35].
Type of digital intervention
The commonly used digital technology for older adults in the reviewed studies were information, assistive and communication types of technology. Seven studies implemented information type of technology (i.e., website program, digital learning platform) to deliver educational content influencing older adult’s knowledge, awareness, lifestyle, physical activities, and cognition [6, 13, 17, 22, 33, 35, 43]. Five studies incorporated an assistive type of technology (i.e., computer, mobile application, smart home device) to support the well-being of people with health conditions, reduce health risks and physical inactivity of older adults and observe the impact of the technology on persons’ cognitive function over time [3, 18, 19, 27, 35]. Three studies utilised communication technology (i.e., video calls and social media platforms) to reduce social isolation, language decline of older migrants, care dependency and health service communication [4, 13, 42]. Three studies appeared to include hybrid-type technology, including both assistive and communication types [18], communication and information types [13] or assistive and information types [35]. Figure 2 summarises types of digital technology and the targeted health areas.

Types of digital technology and the targeted health areas. ˅ = Improved by the digital intervention. ˟ = No improvement by the digital intervention. * = Significant improvement p<0.001 in meta-analysis . % = Number of technology types used in the studies converted into percentage
Effectiveness of digital intervention for healthy ageing and cognitive health
Studies that use digital technology to facilitate healthy ageing in older adults can be summarised into the improved health knowledge and increased physical activities but had no change in health risk reduction and care independence. Studies that use digital technology for cognitive health found it to maintain the cognitive function of older adults when using digital devices (e.g., laptops or cellphones) or engaging in computer-based physical activities in the longer term. There were also improved dementia risk scores from cardiovascular risk reduction and improved depression, anxiety and the associated risks for dementia from the digital programs. The following sections synthesise the review findings from the quantitative and mixed-method studies and meta-analysis.
Health knowledge for healthy behaviour
Online training programs and digital learning platforms were utilised to promote health knowledge, healthy behaviour, digital literacy and competency [6, 17]. Compared to the conventional method of content delivery (face-to-face), older adults in the digital format group had increased ability in health information search (p<0.01), knowledge of nutrition status (p<0.05) and adaptation to ageing (p<0.05) [17]. Digital health literacy examined by the eHealth literacy scale in Bevilacqua et al. [6] also showed a statistically significant improvement in participants’ health knowledge after the digital training program (p=0.001). However, the overall satisfaction with Bevilacqua et al. [6] online training program was not statistically significant (p=0.107). The increased knowledge to health behaviour and mental health were not statistically significant in Hsu et al. [17] digital program. The pooled effect of these two digital programs [6, 17]on health knowledge to healthy behaviour showed not statistically significant (I2 =76, p=0.436, 95% CI [-0.32,0.74]) (see Fig. 3).
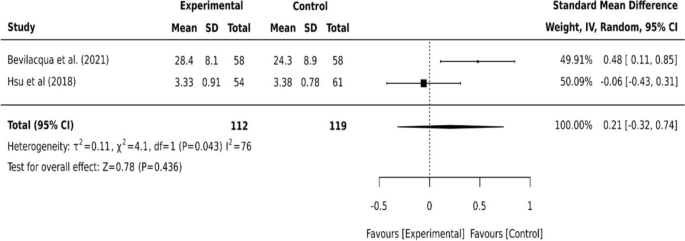
Continuous data for health knowledge to successful ageing
Physical activities and health risk reduction
Digital devices were incorporated into online training programs to increase older adults’ physical activity and reduce cardiovascular-related health risks and the risk of care dependency [13, 17, 27, 35]. A wearable tracker with a smartphone application increased older adults’ engagement in their daily physical activities [27]. However, the digital education program to improve regular exercise by Hsu et al. [17] did not show statistically significant (p=0.084). For health risk reduction, older adults in the coach-supported internet platforms had no statistically significant effect on cardiovascular risk (p=0.10) and lifestyle change to physical activity was also not statistically significant (p=0.34) [35]. The progression in long-term care grade indicating a risk of care dependency of older adults was not statistically significant after the multi-component care approach [13]. The pooled effect of the two studies [13, 35] on reducing cardiovascular-related health risks and care dependency was not statistically significant (I2=0, p=0.426, 95% CI [0.90,1.29]) (see Fig. 4).
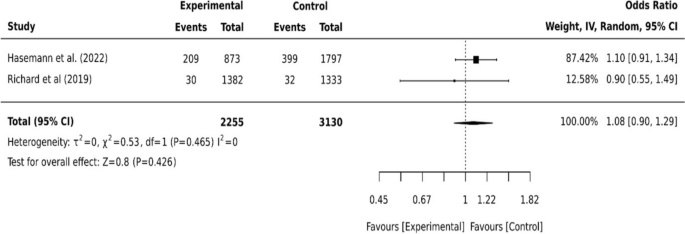
Dichotomous data for cardiovascular risks and care dependency
Cognitive health
Digital technology has been utilised to maintain the cognitive health of older adults including slowing cognitive decline and reducing the risk of dementia development [17, 19, 22, 35, 43]. The longitudinal cohort study that observed participants over 8 years using cellphones and desktop devices showed some degree of influence on people’s cognitive functions [19]. The effect of both devices was not statistically different in the 2-year follow-up (p=0.30) but different statistically significant in the 4-year follow-up (p<0.01) [19]. The study also found different cognition effects between using a cellphone device alone or combined with desktop computer users (p<0.01) [19]. In a computer-based digital inclusion with a physical activity program, older adults had an increased score in the Montreal Cognitive Assessment (MoCA) (p<0.001) and Mini-Mental State Examination (MMSE) (p=0.022) over the 4-month follow-up [43]. However, participants with mild cognitive impairment (Clinical Dementia rating (CDR): 0.5) (n=51) showed no statistically significant change (p=0.600) [43]. The pooled effect of these two digital interventions [19, 43] on older adults’ cognitive health showed a statistically significant improvement (I2=0, p<0.001, 95% CI [0.01, 0.21]) (see Fig. 5).
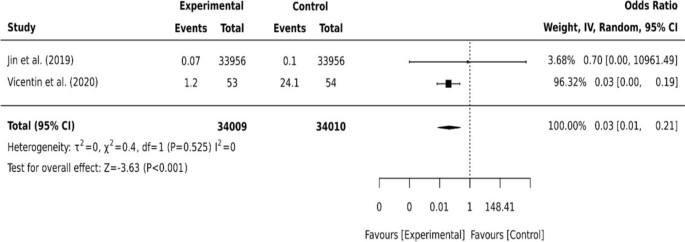
Dichotomous data for two studies on cognition
Other cognitive health studies have shown various outcomes [17, 22, 35]. A virtual cognitive health program did not show a statistical difference in cognition scores at a 24-week follow-up when measured by Repeatable Battery for the Assessment of Neuropsychological Status scores (RBANS) (p=0.15). However, a statistically significant increase in participant cognition was reported at 52 weeks (p<0.01) [22]. The secondary effect of the program on older adult’s depression, anxiety and risk of developing dementia also differed statistically significantly from baseline to week 52 (p<0.01) [22]. In Richard et al. [35], older adults’ dementia risk scores from the Cardiovascular risk factors, Ageing and Incidence of Dementia (CAIDE) showed a statistically significant improvement after the coach-supported internet platform intervention (p=0.02). Cognitive health improved in Hsu et al. [17] following digital program intervention, however, it was not statistically significant (p=0.132). The variation of the intervention outcomes showed between different timeframes. The pooled effect of these three studies [17, 22, 35] on older adults’ cognitive health was not statistically significant (I2=99, p=0.7, 95% CI [-2.27, 1.52]) (see Fig. 6).
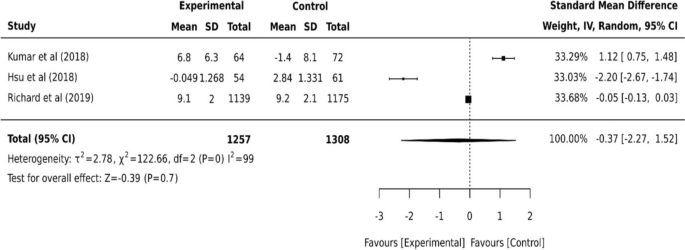
Continuous data for three studies on cognition
Considerations of the digital application to older adults
Thematic analysis was conducted from the qualitative and mixed-method studies and is shown in Table 3. The following sections summarise the emerging themes of digital engagement, communication, independence, human connection, privacy, and cost.
Digital engagement
Digital engagement in this review refers to the extent to which older adults adhere to or interact with digital intervention. Digital literacy/competency, age, motivation and person-centred were identified to influence digital engagement in older adults [18, 27, 33, 42]. Older age has been viewed as a barrier to the extent of a person’s digital device usage [18, 42]. A generational gap in technology use was found in people aged 80 or older with lower or absent use of digital devices compared to those aged 65 and 79 [18]. Older adults were also less confident in their ability to use the digital tool without any assistance [42]. However, individual preferences and choices of person-centred manner drove positive digital engagement [18]. The flexibility of the programs motivated participants to exercise in their own time [33]. Whereas some participants found it difficult to follow with a lack of clear structure [33].
Communication and Independence
Health service communication and the importance of independent living were addressed among older adults [3, 18, 42]. A digital health module that was equipped with a video conferencing feature has enabled older migrants with cancer to communicate with their healthcare providers [42]. Assisted by a smartphone care coordination application, older adults perceived it useful in facilitating communication between patients, family caregivers, and physicians [18]. Additionally, installing a voice control tablet at home for older adults with health conditions enabled them to obtain information and organise personal appointments and medications, positively impacting their independence and reducing stress on carers [3].
Human connection
Social isolation and companionship related to human connection were mentioned among older adults [4, 18]. Using video calls or social media platforms, older adults with migration backgrounds could stay connected and maintain their own social and cultural identities [4]. However, older adults expressed fear of reducing human contact with increased technology use [18]. The robotic devices for companionship were found to infantilise general older adults and deceive people living with dementia [18].
Privacy and cost
Issues were also raised regarding privacy, safety, and the cost of the technology [6, 18, 33]. Collecting personal information in the digital application could be repurposed, leaked, or accessed by a third party [18]. Health insurance does not cover reimbursement of digital health technologies which may result in socioeconomic inequalities and low adoption of digital health technologies [18]. The cost concern of technology was found to impact participants’ satisfaction with the training program significantly [6].
link







