
Empowering frail older adults: multicomponent elastic-band exercises and BCAA supplementation unleash physical health and preserve haematological biomarkers

1. Introduction
Frailty is characterized by a set of physical and cognitive impairments that are related to older adults living in nursing homes who tend to be have more difficult doing the essential daily tasks (1, 2). Europe has one of the highest rates of frailty among institutionalized older adults, with a prevalence of approximately 70%, indicating that frailty is a general characteristic of populations residing in long-term care (3). Despite its high prevalence and potential reversibility when detected and treated early, few studies have specifically focused on institutionalized older adults. This knowledge gap is significant considering the associated poor health outcomes and the urgency to address frailty in this population (4).
Although ageing is recognized as a natural and irreversible degenerative process, current data have shown that regular exercise, especially when accompanied by appropriate nutrition programs, is an efficient non-pharmacological intervention able to retard and (5), to some extent, prevent the fast progression of age-related physical and cognitive impairments. Exercise and nutritional supplements are widely established treatments and preventative measures for frail older adults (6). According to a recently published study (7), frail older adults should be referred to progressive Multicomponent Exercise Programs (MEP) that include resistance, balance, and aerobic training components, as well as multifactorial interventions involving supplementation (8). These interventions have been shown to effectively reduce and delay the onset of frailty while enhancing participants’ functional capacity and health-related quality of life.
According to literature, the multifactorial intervention programs is an innovative approach applied to older populations that includes progressive resistance strength training exercises, balance training for activities of daily living, cardiovascular exercises, and nutritional supplementation (7, 8). Although several dietary supplementation strategies have been investigated in recent years to mitigate the adverse effects of frailty and its related health outcomes (9, 10), the focus has primarily been on interventions incorporating Branched-Chain Amino Acids (BCAAs) and regular exercise (11, 12).
The supplementation with BCAAs, including leucine, valine, and isoleucine, has been suggested as one of the best low-cost strategies to prevent and mitigate motor and mental disabilities associated with aging and frailty (10, 13), particularly when combined with regular exercise programs (5, 7, 8). BCAAs are unique in this regard as they are primarily absorbed by skeletal muscle instead of the liver, making them special (14). The liver indirectly affects BCAA metabolism through the activity of the enzyme “branched-chain ketoacid dehydrogenase” (BCKD), which is known to be reduced in muscle tissue where BCAAs are oxidized (12). Additionally, the enzyme “branched-chain aminotransferase” is responsible for the reversible transamination of BCAAs (14, 15).
Studies have demonstrated that BCAAs play significant roles in enhancing protein synthesis by regulating the mammalian target of rapamycin (mTOR) pathway, serving as both an energy source and a precursor for other amino acids in muscle. BCAAs have also been shown to reduce muscle breakdown and increase protein synthesis (16). Regarding the mTOR mechanism, leucine has been shown to promote increased phosphorylation status of mTOR, inhibiting the action of the Tumour Suppressor Complex (TSC1/TSC2) complex (17). In addition to the administration of BCAAs, resistance exercise is characterized by an increase in growth factors such as insulin-like growth factor 1 (IGF-1), which activates phosphoinositide 3-kinase (PI3-Kinase) and, in turn, stimulates protein kinase B (PKB) expression (17). In turn, PKB can phosphorylate tuberous sclerosis complex 1 (TSC1), leading to a decrease in the production of the TSC1/TSC2 complex. Consequently, this cascade increase protein synthesis through the mTOR pathway and phosphorylation of the p70S6 kinase (18).
In the literature, more than 40 biomarkers of cardiovascular function have already been studied as potential predictors of frailty, although some controversy persists (19, 20). Several scales are currently used by gerontologists to monitor frailty, and the Fried frailty scale or Frailty Phenotype is one of the most accurate and widely used (21). Regarding blood biochemistry, specific blood components such as haemoglobin content (Hb), haematocrit percentage (%Hct), and platelet concentration have also been correlated with frailty and dementia (22). The relationship between lower levels of Hb and the decline of muscular strength and frailty has been analysed and validated by several clinical studies (22, 23). Furthermore, it is also known that higher %Hct or higher blood viscosity (directly associated with the rheostatic properties of blood) have been linked to a higher risk of cardiovascular diseases, insulin resistance, obesity, dyslipidaemia, hypertension, or even mortality (24–27).
Several studies have investigated the effects of exercise combined with BCAA protein supplementation in older adults, revealing significant benefits. The ingestion of leucine-enriched essential amino acids and carbohydrates following resistance exercise was found to enhance mTOR signalling and protein synthesis in human muscle (28). The another study focused on the effects of leucine and its metabolite β-hydroxy-β-methyl-butyrate on human skeletal muscle protein metabolism, showing positive outcomes (29). In a systematic review which examined the prevalence of sarcopenia in aging adults and interventions for its management, the importance of addressing muscle loss in older populations was emphasized (30).
Several studies investigating the effects of regular exercise training and BCAA supplementation in older adults have shown mixed results (31). For instance, a recent one with a same design found that BCAA supplementation did not improve muscle protein synthesis rates in older men during resistance exercise (32, 33). Similarly, a randomized controlled trial previous conducted reported no significant differences in muscle strength or physical function between the exercise plus BCAA supplementation group and the exercise-only group in older individuals (34). These contrasting findings emphasize the complexity of the topic. Besides a slight controversy, optimistic perspectives from recent and solid studies (3, 7) have fuelled the discussion about the efficacy of BCAA supplementation combined with regular exercise in improving the quality of life of older adults. In comparison to isolated supplements, a dietary strategy would therefore be more likely to yield a beneficial outcome in a higher percentage of older adults, especially when combined with MEP.
Therefore, the purpose of this study is to determine the impact of a 40-week multicomponent exercise program on haematological biomarkers and frailty scores in older adults living in residential care homes (RCH), with or without BCAA supplementation. Additionally, we hypothesize that participants’ physical function and cardiovascular systems may be affected by the combination of MEP and BCAAs. Additionally, we hypothesize that the combination of MEP and BCAAs may impact participants’ physical function and cardiovascular systems. Furthermore, we anticipate that there will be no significant changes in the overall status of the elderly during the 8-week period of the withdrawal of interventions.
2. Methods
2.1. Study design and settings
This is a four-phase prospective, naturalistic, controlled clinical trial (treatment vs. care) that includes a washout period (intervention-withdraw-intervention) with a four-arm experimental design (MEP + BCAAs, BCAAs, MEP, and CG). The study involved older adults living in RCH in the city of Coimbra, Portugal, who were 70 years old or older. The recruitment process for engaging institutions in this study has been previously outlined in studies published by our research group (8, 11). The first phase involved a baseline data collection (T1), followed by a 16-week intervention. In the second phase, data collection (T2) was conducted, and an 8-week washout period followed. In Phase 3, the intervention was resumed for another 16 weeks, with a third data collection. After the 16-week intervention period, the final data collection (T4) was conducted. The different stages of exercise and BCAA supplementation are presented in Figure 1.
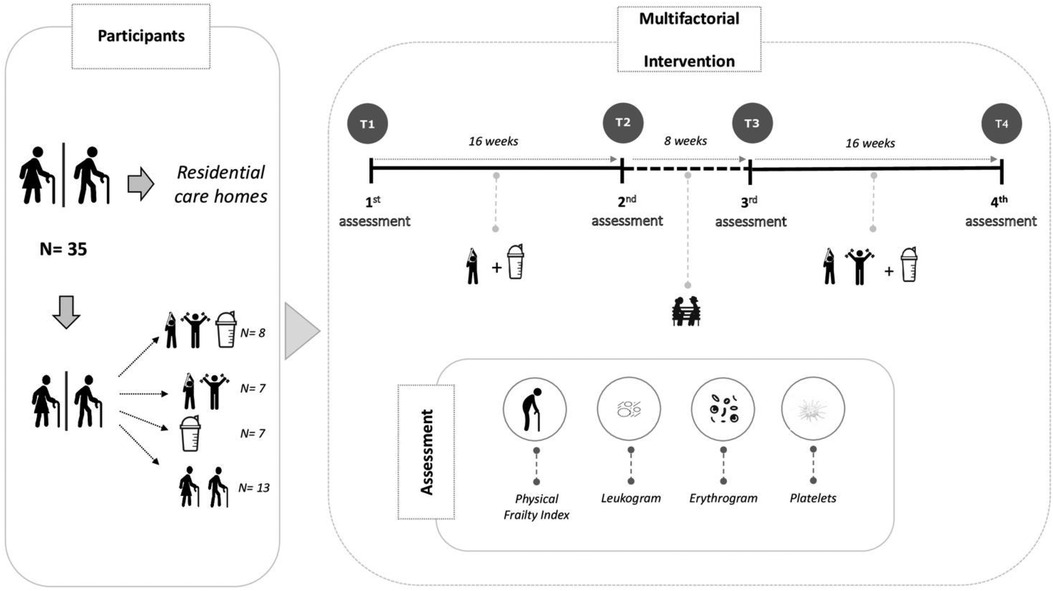
Figure 1. Timeline of the intervention study involving 4 intervention arms and the main indicators analyzed.
2.2. Participants recruitment and allocation
Volunteers’ eligibility, allocation, and experimental design have been fully described in previous studies conducted by our research group (8, 11). Briefly, out of the initially screened 50 volunteers, only 35 participants (83 ± 3 years) completed the 40-week intervention, as detailed in Figure 1. These volunteers were divided into the following groups: Multicomponent Exercise plus Branched Chain Amino Acid supplementation (MEP + BCAA, n = 8); Multicomponent Exercise (MEP, n = 7); Branched Chain Amino Acid supplementation only (BCAA, n = 7); and the non-exercise/no-supplementation control group (CG, n = 13). The guidelines of the Consolidated Standards of Reporting Trials (CONSORT) were followed for all procedures (35).
2.3. Data collection
This study encompasses four assessment points: T1 to T4. Once the experimental groups were established, baseline data was collected at T1, followed by a 16-week period of elastic-band strength training and/or BCAA supplementation, with a subsequent data collection at T2. This initial exercise intervention was succeeded by an 8-week washout period, concluded with a new data collection for detraining/washout analysis at T3. Finally, after the washout period, the strength exercise protocol was replaced by a MEP (including the former elastic band strength exercises, along with aerobic and balance exercises) for an additional 16-week period, culminating in a final data collection at T4 (see Figure 1).
2.4. Ethical statement
The exercise sessions and/or supplementation programs were voluntary for all participants, with a consent form signed by the administrators of the institution, the participants, or their legal representatives before the start of the intervention. This study, approved by the Ethical Committee of Faculty of Sport Sciences and Physical Education, University of Coimbra (reference number: CE/FCDEFUC/00282018), adhered to the Portuguese Resolution (Art. 4th; Law no. 12/2005, 1st series) on ethics in human research (36), and the Helsinki’s Declaration (37). The clinicaltrials.gov registration number for this study is NCT04376463, complementing the newly published article by providing additional biochemical data.
2.5. Outcomes measures
Every evaluation was conducted between 10:00 and 11:45 AM. The initial session aimed to assess the biosocial and overall health status, cognitive profile, nutritional intake, physical condition, and physical frailty status of the volunteers. On the second day, non-fasting blood samples were collected and analysed.
2.5.1. Biochemical analysis
Non-fasting blood samples were collected in the morning (between 10:00 a.m. and 11:00 a.m.) via venipuncture using EDTA-containing tubes at the four checkpoints (T1 to T4), following a 24–48 h period after the last training session. The collection took place in an isolated and quiet room after a 15-minute rest. Prior to blood collection, volunteers were instructed to abstain from alcohol and caffeine consumption and maintain their regular sleep patterns the night before. Immediate blood cell counting was conducted using an automated hematology analyzer, Coulter Act Diff (Beckman Coulter, USA). The following biochemical markers were analyzed: Red Blood Cell Count (Erythrogram), Mean Cell/Corpuscular Volume (MCV), Mean Cell Hemoglobin (MCH), MCHC Mean Cell Hemoglobin Concentration (MCHC), RDW Red Blood Cell Distribution Width (RDW), Haematocrit (HCT), Leukogram (White Blood Cell Count), Lymphocytes, Monocytes, Granulocytes, Platelets (PLT), and Mean Platelet Volume (MPV).
2.5.2. Physical frailty Index
Fried’s of Physical Frailty Phenotype were used (38). Volunteers were categorized as pre-frail if one or two criteria were met, frail if three or more were met, and robust if none of the five physical frailty signs were present (10): (i) Weight loss in volunteers was determined by self-reporting an unintentional weight reduction of at least 4 kilograms in the previous six months; (ii) Self-reported exhaustion was evaluated by agreement on questions number 7 (“I felt that everything I did was an effort”) and 20 (“I could not get going”) from the Center of Epidemiologic Studies for Depression scale (39); (iii) Hand-grip strength was assessed using a hand-held dynamometer (Lafayette 78,010, Sagamore, United States) and the better outcome from two trials was selected for scoring. Volunteers unable to perform the hand-held test and those in the lowest 20% were categorized as positive for that frailty index (40). The cut-off reference values for the hand-held test were ≥29 kg for males and ≥17 kg for female. (iv) Slowness was measured using the “15 feet (4.6 m) walking test”. Scores of times ≥7s for males and ≥6 s for females, based on the cut-off values of Fried’s study population, were considered positive for slowness (38). Final scoring was based on the faster of the two trials; (v) Low physical activity levels were assessed using the short-version of International Physical Activity Questionnaire (41). The questionnaire classified physical activity into three categories: slightly active, very active, and inactive. Volunteers classified as inactive had a positive score for this physical frailty component. In this study, volunteers classified as frail (3 or more points) and pre-frail (2 points) were included in the intervention phase. In order to track the effects of the intervention over time, a continuous measure called the physical frailty total score (0 to 5 points) was used (38), and scores closer to 5 indicating more frailty condition.
2.5.3. Nutritional and general health Status
The nutritional assessment and clinical and health status were conducted as previously described (11). Briefly, the diet was analyzed using specific tools such as photographic quantification of portions and food tables designed for the Portuguese population (42), following the methods of previous studies (43). Additionally, the Portuguese version of Mini Nutritional Assessment (MNA) questionnaire was administered (44). The clinical and health/illness status was evaluated using the Charlson comorbidity index (CCI), which took into account individual comorbidity registration, age, and gender to calculate the final CCI score (45). Anthropometric measurements included body mass (kg) and stature (cm). Body mass was measured using a portable scale (Seca®, model 770, Berlin, Germany) with a precision of 0.1 kg, while stature was determined using a portable stadiometer (Seca Body meter®, model 208, Berlin, Germany) with an accuracy of 0.1 cm. Body mass index (BMI) was calculated using the equation BMI = (body mass)/(stature)². Standardized procedures for these measurements were described in previous studies (46).
2.6. Full characterization of the multifactorial intervention
2.6.1. Oral supplementation with BCAA
The BCAA powder mixture was composed of L-leucine (Leu), L-isoleucine (Ile), and L-valine (Val) in the mass proportion of 2:1:1 (MyProtein®, Cheshire, UK), accounting for 20 kcal per portion. The procedures related to supplement administration were implemented based on prior studies (47–49). An unflavored supplement was used to avoid ingestion preferences for specific flavors by the participants. The BCAA mixture was diluted in 200 ml of water and given immediately after the exercise sessions to the volunteers in the MEP + BCAAs group (47). The supplement dose was fixed at 0.21 g total BCAA/kg/session (48). The supplement dose was set at a total of 0.21 g between 09:00 and 11:30 a.m. in the BCAA group. The BCAA-supplemented (MEP + BCAAs and BCAAs) and BCAA-absent groups (MEP and CG) were split according to the proximity between the RCH, where the exercise programs were effectively applied. No documented interactions between the volunteers from the BCAA-supplemented and no-BCAA supplemented groups in our study.
2.6.2. Multicomponent exercise program
Each session commenced with a brief five-minute warm-up consisting of range-of-motion exercises for the wrists, shoulders, hips, knees, and ankles, as well as walking. The exercise sessions (T1–T2 and T3–T4) were conducted twice a week, with a 36-hour break between sessions to allow for adequate rest and recovery. The exercise protocol adhered to the exercise prescription guidelines for older adults and the exercise periodization guidelines outlined by the American College of Sports Medicine (50). The exercise program for T1–T2 began with a two-week adaptation period, during which seven different exercises were performed using elastic bands (TheraBand®, Hygenic Corporation, Akron, OH, USA). Close supervision was provided to the volunteers during the initial two sessions to familiarize them with the equipment and make adjustments based on their perceived exertion level using the Rating Perceived Exertion scale, also called RPE-OMNI Scale (51). These introductory sessions aimed to educate the volunteers on proper training techniques, as well as assist them in selecting the appropriate elastic band color, length, and grip width.
After the initial two-week adaptation period, the exercise program’s intensity was gradually increased. This involved adding two additional exercises, bringing the total to ten exercises, and incorporating different colored bands based on the OMNI table (35). To ensure safety, the volunteers’ heart rate was monitored during the exercise sessions using Polar M200® (Polar Electro Oy, Kempele, Finland), randomly distributed among participants. The maximum HR (HRmax) was calculated using a specific formula for the older population (52). A low to moderate intensity effort, around 50%–75% HRR, was attained as recommended by the American College of Sport Medicine (50).
The exercise retraining program for T3–T4 also utilized the elastic bands, but it also included a walkability program, adding step exercises, coordination, and balance exercises as well as exercises that replicate physical activities used in daily life such as sitting and rising from the chair. Dumbbells and ankle/wrist weights were occasionally incorporated as well, forming a MEP that lasted for the same 16-week period (twice a week, alternating days, totaling 32 sessions).
2.6.3. Washout and detraining period
During the (T2–T3) period of multifactorial intervention, the volunteers experienced an 8-week detraining and washout phase in which the supplementation and exercise regimens were halted. The objective of this phase was to investigate whether the physiological adaptations achieved during the initial intervention phase were maintained or if an 8-week cessation could lead to a reversal of the hematological, and physical fitness adaptations (53).
2.7. Statistical analysis
The Shapiro-Wilk test was used to verify the normality distribution of the collected data. Descriptive values are expressed as mean ± standard deviation (SD). To compare the mean changes over time between groups, repeated measures ANOVA (4 × 4 group vs. time) were performed. Bonferroni’s post-hoc analysis was performed for paired comparisons of means when significant interactions were found in the dependent variables (Leukogram, Erythrogram, Platelets), and confidence intervals (CI: 95%) were reported when a significant effect was found. The level of significance was set at p < 0.05. All statistical analysis were done using IBM SPSS Statistics version 23.0 (Armonk, NY: IBM Corp, USA).
3. Results
Despite one isolated case of diarrhea (following the first BCAA supplementation), in which the participant quickly recovered and resumed the protocol without further issues, no other adverse events, injuries, or intervention-related complications were observed throughout the study. Authorized data obtained from RCH nurses revealed that 68% of the volunteers were using cardiovascular disease medications (atorvastatin/simvastatin). Please refer to Table 1 for more details.
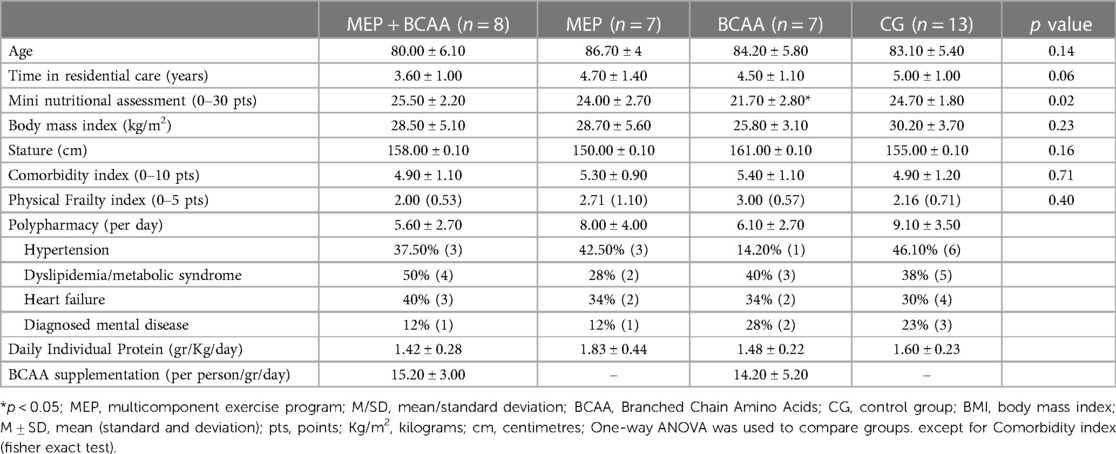
Table 1. Characteristics of experimental and control groups at baseline.
3.1. Red blood cell count (erythrogram)
The values of the markers Erythrogram indexes for the different intervention groups before and after the multifactorial intervention are shown in Table 2. An important finding of the time*group interaction was observed for MCH (Mean Cell Hemoglobin) [F(df: 6.058, 34.32) = 4.200, p = 0.003]. Bonferroni comparisons revealed baseline differences between the ME + BCAA and BCAA groups (CI: −9.49, −0.04, p = 0.04). However, over time, significant changes were only observed in the ME + BCAA group between T1 and T2 (CI: −3.628, −0.806, p = 0.001), and in the CG (Control Group) between T2 and T4 values (CI: −3.12, −0.08, p = 0.03).
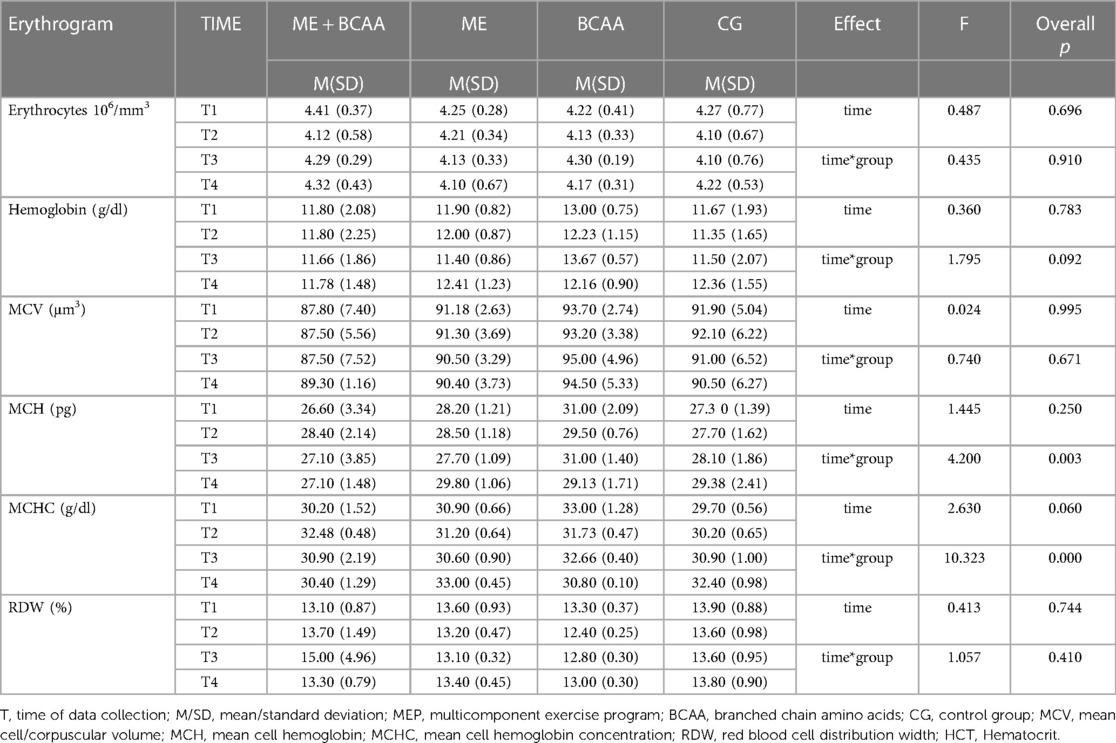
Table 2. Erythrogram indexes of the different intervention groups before-after multifactorial intervention (T1–T4).
Significant effects of time*group interaction were found for MCHC (Mean Cell Hemoglobin Concentration) [F(df: 9, 51) = 10.323, p < 0.001]. Bonferroni post hoc analysis showed that, in a similar way for MCH results, the baseline values of MCHC parameter in BCAA group was higher than the ME + BCAA group (CI: −5.218, −0.749, p = 0.006). At T2, CG showed lower MCHC values in comparison to all other groups (p < 0.001, p = 0.035, p = 0.011, for ME + BCAA, ME, and BCAA groups, respectively). While for T3 no differences emerged between groups, at the last follow-up (tT4) ME group presented the higher MCHC levels in comparison to ME + BCAA group (CI: 1.017, 4.183, p = 0.001) and BCAA group (CI: 0.261, 4.139, p = 0.021). MCHC levels also differ between the groups CG and ME + BCAA in the same time point (CI: 0.417, 3.583, p = 0.009). In addition, over time, significant differences were found between T1 and T2 (CI: −3.685, −1.182, p < 0.001), T2 and T3 (CI: 0.69, 3.064, p = 0.037), as well as T2 and T4 (CI: 0.839, 3.328, p = 0.001) in the ME + BCAA group. Furthermore, in the ME group, the MCHC values at T4 were significantly higher compared to T1 (CI: 0.689, 3.477), T2 (CI: 0.489, 2.978), and T3 (CI: 0.975, 3.658; p < 0.05 for all). The BCAA group also showed a significant difference in MCHC between T1 and T4 (p < 0.05), while no significant changes were observed at other checkpoints in the same group. Additionally, the CG exhibited an increase in MCHC over time, with the highest values obtained at T4 compared to T1 (CI: 1.239, 4.027), T2 (CI: 0.955, 3.445), or T3 (CI: 0.158, 2.842) (p < 0.05 for all).
3.2. White blood cell count (leukogram)
The values of the markers Leukogram indexes for the different intervention groups before and after the multifactorial intervention are shown in Table 3. No significant changes for time and time*group interactions were found for other parameters of RBC (T1-T4).
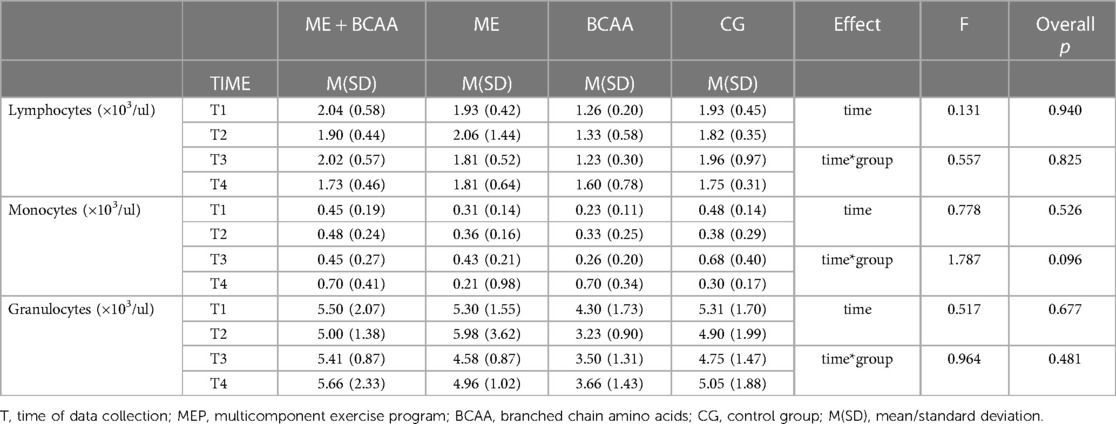
Table 3. Leukogram indexes of the different intervention groups before-after multifactorial intervention (T1–T4).
3.3. Platelets
The values of the markers Platelets indexes for the different intervention groups before and after the multifactorial intervention are shown in Table 4. Regarding platelets, no significant effect of time or time*group interactions were observed in any of the evaluated indexes (p > 0.05).
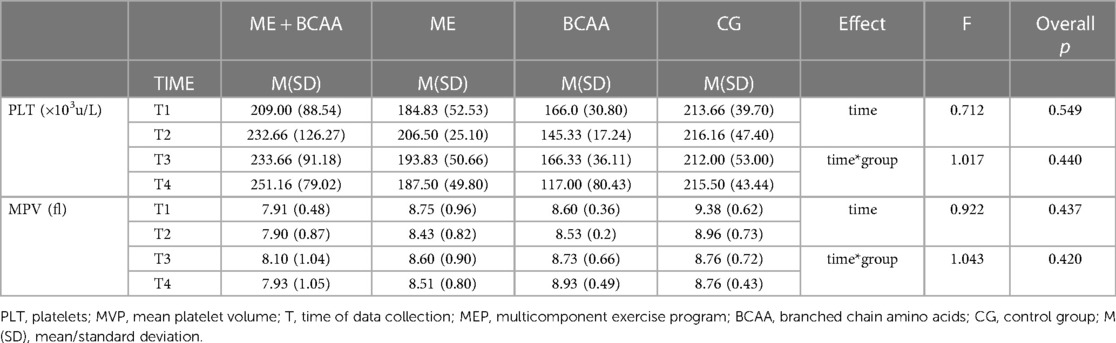
Table 4. Platelets indexes of the different intervention groups before-after multifactorial intervention (T1–T4).
3.4. Physical frailty
A significant interaction between time vs. group was observed for the frailty index (F = 3.799, p = 0.001). No significant differences between groups were found at T1, T2, and T3. However, at the final follow-up (T4), the CG exhibited higher levels of frailty compared to both the MEP + BCAA and BCAA groups (p = 0.008 and p = 0.012, respectively). As depicted in Figure 2, over time, the BCAA group exhibited a notable reduction in the frailty index from T1 to T2 (p = 0.005). In contrast, the Control Group experienced a slight increase in frailty during each follow-up, leading to a significant difference between T1 and T4 (p < 0.001).
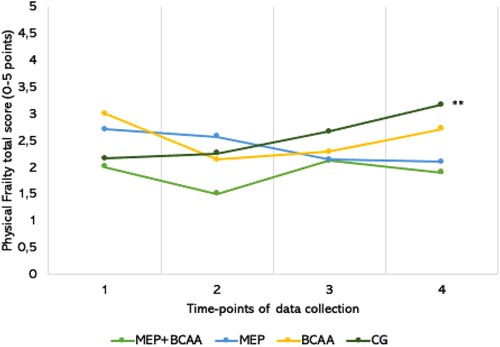
Figure 2. **p < 0.001; the total frailty scores-variation of all intervention groups in the 40-week of multifactorial intervention, that consisting of 16 weeks of intervention (T1–T2), an 8-week withdrawal period (T2–T3), and another 16 weeks of intervention (T3–T4).
4. Discussion
Taken into account that the goal of this study was to determine the impact of a 40-week MEP on hematological biomarkers and physical frailty scores in older adults living in residential care homes (RCH), supplemented or not with BCAA, the results obtained corroborated our initial hypothesis that the MEP, particularly when combined with BCAA supplementation, could lead to improvements in hematological biomarkers, as well as in physical frailty.
In fact, our findings demonstrated that intervention with MEP was able to ameliorate the overall frailty levels of the participants, indicating that this exercise training program, especially when combined with BCAAs supplementation, effectively can contribute to reducing physical frailty in older adults. Additionally, the results concerning MCH and MCHC parameters allow us to putatively suggest that the interventions applied in the present study have positively impacted the erythrocyte concentration and hemoglobin levels, in a similar way as formerly reported when the exercise training was combined with BCAA supplementation (54). These results support the notion that a comprehensive approach incorporating both exercise and nutritional interventions can yield significant benefits in mitigating physical frailty and improving hematological parameters in older adults.
4.1. Hematological changes
In relation to the hematological parameters assessed here, it was possible to observe significant differences in the time*group analysis only in the MCH and MCHC values. In this respect, it is worth pointing out that the baseline differences found in these parameters between the BCAA group and ME + BCAA group could be attributed to the nutritional status since a similar result was observed in the Mini Nutritional Assessment (MNA). In accordance with the literature, some factors, such as aging, chronic inflammation, and nutritional status can influence the red blood cell distribution (55, 56), which includes the MCH and MCHC parameters. At this point, it is paramount to mention that the statistically significant differences in the baseline nutritional status between these groups could be associated with the randomization process of the volunteer groups. It is well-known that these variations in nutritional status can not only reflect diverse dietary habits and lifestyle factors according to socioeconomic status (57), but also influence the volunteers’ overall health and physical condition, which contributes to the development of frailty (58). Therefore, addressing and exploring these differences could be useful to provide valuable insights into the intricate relationship between nutrition, exercise, and frailty in older adults.
Beyond the baseline significant differences, specifically, the MCHC values found in the 3 groups submitted to a type of intervention were higher than the values found in the control group at the T2 time point. In a general way, the increased MCHC values can represent an elevation of the concentration of hemoglobin inside the red blood cells (RBC), or, alternatively, that hemoglobin is found outside of the RBC due to its destruction. Since the normal range of MCHC is around 29 to 35 g/dl, our results demonstrated that all volunteer groups maintained their MCHC level in normal conditions during the study period. Therefore, we can suggest that the increase of MCHC at the T2 time point in the MEP, MEP + BCAA, and BCAA groups can indicate that both the exercise training program and BCAA supplementation were able to improve the bioavailability of oxygen to tissues. In fact, it is worth citing that regular endurance training can accelerate the removal of the oldest RBCs, which induces the production of new RBCs (59). Thus, in line with these pieces of information, the MEP applied in the present study, by including aerobic training, could putatively contribute to the elevation of MCHC values by favoring the RBCs removal and, consequently, the generation of new cells with more hemoglobin quantity in order to improve oxygen-carrying capacity leading to the better tissue oxygenation. In a different way, older adults submitted to a MEP intervention during acute hospitalization did not present alteration in the RDW levels (56).
Despite the effect of BCAA supplementation on hematological parameters is still scarce in the literature, it was reported that BCAA supplementation increased not only the RBCs number and hematocrit, as well as the hemoglobin levels in outpatients with liver cirrhosis (60). Particularly in the older adult population, it was documented that an improvement in the oxygen-carrying capacity by RBCs was attributed to the combined effect of exercise and BCAA supplementation (15, 16). These findings align with the notion that the MEP, when combined with BCAA supplementation, can exert a beneficial influence on hematological parameters, contributing to the overall well-being of older adults (30, 32).
In an interesting way, a formerly research demonstrated that BCAA supplementation improved muscle mass in cirrhotic patients with sarcopenia (61). Additionally, another study showed that BCAA supplementation improved the liver frailty index in frail compensated cirrhotic patients (62, 63). These findings support the notion that BCAAs have a positive impact on muscle mass and functional outcomes in older adults. Additionally, our group also showed that exercise interventions combined with BCAA supplementation can modulate inflammatory markers and enhance muscle strength and power (11, 48).
Based on the report that there is a positive association between hemoglobin concentration and physical performance, the importance of optimizing hematological parameters for maintaining overall physical function in older adults is emphasized (64). Future studies should consider exploring the long-term effects of MEP and BCAA supplementation on various health outcomes, including innovative myokines as biomarkers related to immune function. These findings have practical implications for the development of exercise and nutritional interventions aimed at improving physical frailty and hematological biomarkers in older adults, ultimately enhancing their overall well-being and quality of life.
Concerning the results related to the different time points assessed here (intragroup analysis), since the alterations observed in both MCH and MCHC parameters were, in a general way, similar between the volunteer groups, we can putatively suggest that these findings were attributed to the seasonal variation. In fact, it has been demonstrated that the hematological parameters are closely influenced by the seasonal variation in different populations, including athletes and healthy individuals (65–67). Interestingly, it was evidenced that hematocrit and hemoglobin levels decrease in the summer due to the hemodilution (65, 66), and/or increase in the winter due to the hemoconcentration (68).
Platelets are the lowest cellular components in blood. The activation of platelets for further degranulation and aggregation is fundamental for blood haemostasias and are mediated by several specific platelet-stimulating mediators, such as α-Granules (69–71). Nevertheless, no significant changes in platelet distribution were observed here with exercise and/or BCAA supplementation of older individuals. However, studies already published by other groups showed significant differences between the active and the inactive groups regarding platelet scores. Sample size, the experimental groups (anthropometric values, age, inactivity, etc.), and logistic specificities of our study could explain such discrepancies.
The statistically significant differences in the nutritional profile at baseline between the study groups have some implications for the results interpretation. These variations can impact the absorption and utilization of BCAA supplementation, potentially affecting its effectiveness in combination with MEP (72). Moreover, differences in nutritional status may influence the participants’ overall health and physical condition, contributing to frailty and confounding the intervention effects (58). It is crucial to acknowledge these baseline differences when discussing the study findings and their implications. Additionally, the variations in nutritional profile reflect diverse dietary habits and lifestyle factors according the socioeconomic status (57), which can significantly influence health outcomes and interact with the interventions under investigation.
4.2. Impact on frailty status
Frailty in the MEP group showed a tendency to decrease over time, indicating the positive effects of exercise. Significant reduction in frailty was observed only during the initial 16 weeks of treatment with BCAA supplementation. Similarly, the MEP + BCAA group exhibited a similar pattern, further confirming the beneficial impact of BCAA supplementation in combination with exercise. These findings underscore the effectiveness of the exercise program, particularly when combined with BCAA supplementation, in reducing physical frailty in older adults residing in RCH (73). Institutionalization is a psychosocial event experienced by individuals during different stages of their lives, providing social and health protection (74). The British Geriatric Society emphasizes the importance of regular procedures and agreed-upon measurements in social and health care relationships with older adults to screen for frailty, including sarcopenia. These recommendations underscore the significance of adopting an active lifestyle, and dietary protein intake, as a strategy to mitigate the negative consequences of physical frailty and prevent its progression to more severe conditions (75, 76).
The outcomes of our study align with previous research highlighting the potential of non-pharmacological interventions, such as exercise programs, to address physical frailty and sarcopenia in older individuals (77). In the same direction, the study involving the same population on chair-based exercise programs in institutionalized older women highlighted the positive effects of such interventions on salivary steroid hormones, disabilities, and frailty changes, further supporting the benefits of exercise programs in improving health outcomes in older adults (78). Based on these findings, we suggest that exercise, BCAA supplementation, or their combination could potentially ameliorate frailty in institutionalized older individuals. It is noteworthy that the control group was the only group that experienced a notable decline in frailty status, highlighting the importance of interventions in preventing frailty progression. Institutionalization provides an opportunity for health protection. Non-pharmacological interventions, like exercise and diet programs, are effective in addressing frailty. Prevention is crucial to halt frailty progression.
4.3. Limitations, novel and directions for future studies
The study had limitations including a small sample size, lack of diversity, and a relatively short intervention duration. The small sample size may limit the generalizability of the findings and statistical power. The focus on frail older adults in nursing homes may not represent the broader population, suggesting the need for more diverse samples. The 40-week intervention duration might not have been long enough to observe significant changes in hematological markers, indicating the importance of longer intervention periods for better understanding the effects of BCAA supplementation and exercise. The novelty of the study lies in the combination of BCAA supplementation and MEP. This unique approach contributes to the existing literature by investigating the effects of this combination on hematological indicators in frail older adults. The study adds to the current understanding of the potential benefits of BCAA supplementation and exercise by examining their combined effects, providing valuable insights into the efficacy of this novel intervention strategy.
Our findings align with real-world data reflecting the challenges faced in nursing homes, where participants exhibit various impairments, comorbidities, and motivational obstacles. Conducting a 40-week controlled study with this population is subject to additional limitations, such as unforeseen factors like mortality or changes in nursing home residency. Future studies should focus on long-term follow-up assessments to determine the sustained effects of BCAA supplementation and exercise interventions on hematological markers and physical frailty in older adults. Additionally, mechanistic investigations are needed to explore the underlying physiological mechanisms involved. Comparisons with other interventions and investigations into individual differences in treatment response should also be considered to enhance our understanding and personalize interventions for older adults.
4.4. Practical applications
The practical purposes of our study are twofold. Firstly, the combination of BCAA supplementation and MEP can be considered as a potential non-pharmacological intervention for improving the hematological indicators and physical frailty of older adults residing in nursing homes. This suggests that healthcare professionals and caregivers can incorporate these interventions into the care plans of frail older adults to enhance their overall well-being. Secondly, our study highlights the importance of long-term follow-up assessments and personalized interventions that consider individual differences to optimize the efficacy of BCAA supplementation and exercise programs in this population. This knowledge can guide future research and clinical practice in promoting healthy aging and improving the quality of life for older adults in residential care settings.
5. Conclusion
Our study provides valuable insights into the effects of BCAA supplementation and a MEP on hematological indicators and physical frailty in older adults residing in nursing homes. Although the long-term intervention did not result in significant changes in the hematological profile, the combination of BCAA supplementation and MEP demonstrated potential pro-immune effects and maintained certain hematological markers. These findings contribute to the existing literature by examining the effectiveness of these interventions in frail older adults, emphasizing the importance of incorporating exercise and nutritional strategies for promoting healthy aging. Moreover, our study aligns with the Sustainable Development Goal 3, as it addresses the objective of ensuring good health and well-being for older adults. Personalized interventions, long-term follow-up assessments, and consideration of individual differences can optimize the efficacy of interventions, improving health outcomes and well-being for frail older adults in residential care settings.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving humans were approved by University of Coimbra, Faculty of Sport Sciences and Physical Education Ethical Committee (reference number: CE/FCDEFUC/00282018). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AS-C and GEF drafted the paper. FD, RSN and GEF helped with data acquisition. RVN and MUC statically analysed the data. AT and AlM developed the study the proposal, revised the manuscript critically and suggested additional statistical analyses. AT and AlM coordinated the research study and, together with MPB, ALB, AnM and FB helped with discussion, and revised the manuscript critically. All the authors approved the final version of the manuscript.
Funding
MPB was supported by São Paulo Research Foundation (FAPESP, grant no 2017/06032-2), and National Council of Scientific and Technology Development (CNPq: PQ-2 #311839/2021-5, Brazil). AB was supported by São Paulo Research Foundation (FAPESP, grants no 10/50025-1, 2016/04845-3, and 2019/14115-0), and National Council of Scientific and Technology Development (CNPq, grant no 307674/2017-7. “Guilherme Furtado” thanks the National funding by FCT- Foundation for Science and Technology, P.I., through the institutional scientific employment program-contract (CEECINST/00077/2021).
Acknowledgments
We would like to thank the Residential Care Homes (RCH) that accepted to participate in this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at:
References
1. Ruan Q, Yu Z, Chen M, Bao Z, Li J, He W. Cognitive frailty, a novel target for the prevention of elderly dependency. Ageing Res Rev. (2015) 20:1–10. doi: 10.1016/j.arr.2014.12.004
PubMed Abstract | CrossRef Full Text | Google Scholar
2. Walston J, Hadley EC, Ferrucci L, Guralnik JM, Newman AB, Studenski SA, et al. Research agenda for frailty in older adults: toward a better understanding of physiology and etiology: summary from the American geriatrics society/national institute on aging research conference on frailty in older adults. J Am Geriatr Soc. (2006) 54(6):991–1001. doi: 10.1111/j.1532-5415.2006.00745.x
PubMed Abstract | CrossRef Full Text | Google Scholar
3. Abizanda P, Romero L, Sánchez-Jurado PM, Martínez-Reig M, Gómez-Arnedo L, Alfonso SA. Frailty and mortality, disability and mobility loss in a spanish cohort of older adults: the FRADEA study. Maturitas. (2013) 74:54–60. doi: 10.1016/j.maturitas.2012.09.018
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Sergi G, Veronese N, Fontana L, De Rui M, Bolzetta F, Zambon S, et al. Pre-Frailty and risk of cardiovascular disease in elderly men and women. J Am Coll Cardiol. (2015) 65:976–83. doi: 10.1016/j.jacc.2014.12.040
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Coelho-Júnior HJ, Milano-Teixeira L, Rodrigues B, Bacurau R, Marzetti E, Uchida M. Relative protein intake and physical function in older adults: a systematic review and meta-analysis of observational studies. Nutrients. (2018) 10:1–16. doi: 10.3390/nu10091330
CrossRef Full Text | Google Scholar
6. Landi F, Calvani R, Tosato M, Martone AM, Ortolani E, Savera G, et al. Protein intake and muscle health in old age: from biological plausibility to clinical evidence. Nutrients. (2016) 8:1–12. doi: 10.3390/nu8050295
CrossRef Full Text | Google Scholar
7. Chiu TY, Yu HW. Associations of multicomponent exercise and aspects of physical performance with frailty trajectory in older adults. BMC Geriatr. (2022) 22:1–10. doi: 10.1186/s12877-022-03246-6
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Caldo-Silva A, Furtado GE, Chupel MU, Bachi ALL, de Barros MP, Neves R, et al. Effect of training-detraining phases of multicomponent exercises and BCAA supplementation on inflammatory markers and albumin levels in frail older persons. Nutrients. (2021) 13:2–17. doi: 10.3390/nu13041106
CrossRef Full Text | Google Scholar
9. Morante JJ H, Martínez CG, Morillas-Ruiz JM. Dietary factors associated with frailty in old adults: a review of nutritional interventions to prevent frailty development. Nutrients. (2019) 11:1–13. doi: 10.3390/nu11010102
CrossRef Full Text | Google Scholar
10. Morley JE, Vellas B, van Kan GA, Anker SD, Bauer JM, Bernabei R, et al. Frailty consensus: a call to action. J Am Med Dir Assoc. (2013) 14:392–7. doi: 10.1016/j.jamda.2013.03.022
PubMed Abstract | CrossRef Full Text | Google Scholar
11. Caldo-Silva A, Furtado GE, Chupel MU, Letieri RV, Valente PA, Farhang M, et al. Effect of a 40-weeks multicomponent exercise program and branched chain amino acids supplementation on functional fitness and mental health in frail older persons. Exp Gerontol. (2021) 155:392–7. doi: 10.1016/j.exger.2021.111592
CrossRef Full Text | Google Scholar
13. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European working group on sarcopenia in older people. Age Ageing. (2010) 39:412–23. doi: 10.1093/ageing/afq034
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Breiding MJ. Branched chain amino acids. Physiol Behav. (2014) 63:1–18. doi: 10.1146/annurev-physiol-020518-114455.Branched
CrossRef Full Text | Google Scholar
15. Shimomura Y, Honda T, Shiraki M, Murakami T, Sato J, Kobayashi H, et al. Branched-chain amino acid catabolism in exercise and liver disease. J Nutr. (2006) 136:250S–3S. doi: 10.1093/jn/136.1.250s
PubMed Abstract | CrossRef Full Text | Google Scholar
16. Neishabouri SH, Hutson SM, Davoodi J. Chronic activation of mTOR complex 1 by branched chain amino acids and organ hypertrophy. Amino Acids. (2015) 47:1167–82. doi: 10.1007/s00726-015-1944-y
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Mohta S, Anand A, Sharma S, Qamar S, Agarwal S, Gunjan D, et al. Randomised clinical trial: effect of adding branched chain amino acids to exercise and standard-of-care on muscle mass in cirrhotic patients with sarcopenia. Hepatol Int. (2022) 16:680–90. doi: 10.1007/s12072-022-10334-7
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Cuthbertson DJ, Babraj J, Smith K, Wilkes E, Fedele MJ, Esser K, et al. Anabolic signaling and protein synthesis in human skeletal muscle after dynamic shortening or lengthening exercise. Am J Physiol Endocrinol Metab. (2006) 290:731–8. doi: 10.1152/ajpendo.00415.2005
CrossRef Full Text | Google Scholar
20. Fontana L, Addante F, Copetti M, Paroni G, Fontana A, Sancarlo D, et al. Identification of a metabolic signature for multidimensional impairment and mortality risk in hospitalized older patients. Aging Cell. (2013) 12:459–66. doi: 10.1111/acel.12068
PubMed Abstract | CrossRef Full Text | Google Scholar
21. Cesari M, Gambassi G, Van Kan GA, Vellas B. The frailty phenotype and the frailty index: different instruments for different purposes. Age Ageing. (2014) 43:10–2. doi: 10.1093/ageing/aft160
PubMed Abstract | CrossRef Full Text | Google Scholar
22. Steinmeyer Z, Delpierre C, Soriano G, Steinmeyer A, Ysebaert L, Balardy L, et al. Hemoglobin concentration; A pathway to frailty. BMC Geriatr. (2020) 20:1–10. doi: 10.1186/s12877-020-01597-6
CrossRef Full Text | Google Scholar
23. Méndez-Giménez A, Fernández-Río J, Cecchini-Estrada JA. Validación de la versión en español del cuestionario de metas de amistad en educación física. Univ Psychol. (2014) 13:227–37. doi: 10.11144/Javeriana.UPSY13-1.vvec
CrossRef Full Text | Google Scholar
24. Danesh J, Collins R, Peto R, Lowe GDO. Haematocrit, viscosity, erythrocyte sedimentation rate: meta-analyses of prospective studies of coronary heart disease. Eur Heart J. (2000) 21:515–20. doi: 10.1053/euhj.1999.1699
PubMed Abstract | CrossRef Full Text | Google Scholar
25. Schreijer AJM, Reitsma PH, Cannegieter SC. High hematocrit as a risk factor for venous thrombosis. Cause or innocent bystander? Haematologica. (2010) 95:182–4. doi: 10.3324/haematol.2009.017285
PubMed Abstract | CrossRef Full Text | Google Scholar
26. Gagnon DR, Zhang TJ, Brand FN, Kannel WB. Hematocrit and the risk of cardiovascular disease-the framingham study: a 34-year follow-up. Am Heart J. (1994) 127:674–82. doi: 10.1016/0002-8703(94)90679-3
PubMed Abstract | CrossRef Full Text | Google Scholar
27. Zierk J, Krebs A, Rauh M, Metzler M, Löscher A, Strasser E, et al. Blood counts in adult and elderly individuals: defining the norms over eight decades of life. Br J Haematol. (2020) 189:777–89. doi: 10.1111/bjh.16430
PubMed Abstract | CrossRef Full Text | Google Scholar
28. Dreyer HC, Drummond MJ, Pennings B, Fujita S, Glynn EL, Chinkes DL, et al. Leucine-enriched essential amino acid and carbohydrate ingestion following resistance exercise enhances mTOR signaling and protein synthesis in human muscle. Am J Physiol Endocrinol Metab. (2008) 294(2):E392–400. doi: 10.1152/ajpendo.00582.2007
PubMed Abstract | CrossRef Full Text | Google Scholar
29. Wilkinson DJ, Hossain T, Hill DS, Phillips BE, Crossland H, Williams J, et al. Effects of leucine and its metabolite β-hydroxy-β-methylbutyrate on human skeletal muscle protein metabolism. J Physiol. (2013) 591:2911–23. doi: 10.1113/jphysiol.2013.253203
PubMed Abstract | CrossRef Full Text | Google Scholar
30. Lozano-Montoya I, Correa-Pérez A, Abraha I, Soiza RL, Cherubini A, O’Mahony D, et al. Nonpharmacological interventions to treat physical frailty and sarcopenia in older patients: a systematic overview—the SENATOR project ONTOP series. Clin Interv Aging. (2017) 12:721–40. doi: 10.2147/CIA.S132496
PubMed Abstract | CrossRef Full Text | Google Scholar
31. Marcon M, Zanella PB. The effect of branched-chain amino acids supplementation in physical exercise: a systematic review of human randomized controlled trials. Sci Sports. (2022) 37:393–404. doi: 10.1016/j.scispo.2021.05.006
CrossRef Full Text | Google Scholar
32. Ko CH, Wu SJ, Wang ST, Chang YF, Chang CS, Kuan TS, et al. Effects of enriched branched-chain amino acid supplementation on sarcopenia. Aging. (2020) 12:15091–103. doi: 10.18632/aging.103576
PubMed Abstract | CrossRef Full Text | Google Scholar
33. Katsanos CS, Kobayashi H, Sheffield-Moore M, Aarsland A, Wolfe RR. A high proportion of leucine is required for optimal stimulation of the rate of muscle protein synthesis by essential amino acids in the elderly. Am J Physiol Endocrinol Metab. (2006) 291:381–7. doi: 10.1152/ajpendo.00488.2005
CrossRef Full Text | Google Scholar
34. Solerte SB, Gazzaruso C, Bonacasa R, Rondanelli M, Zamboni M, Basso C, et al. Nutritional supplements with oral amino acid mixtures increases whole-body lean mass and insulin sensitivity in elderly subjects with sarcopenia. Am J Cardiol. (2008) 101:69E–77E. doi: 10.1016/j.amjcard.2008.03.004
PubMed Abstract | CrossRef Full Text | Google Scholar
35. Des Jarlais DC, Lyles C, Crepaz N. Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: the TREND statement. Am J Public Health. (2004) 94:361–6. doi: 10.2105/AJPH.94.3.361
PubMed Abstract | CrossRef Full Text | Google Scholar
36. Braga BR. Ética na publicação de trabalhos científicos. Rev Port Med Geral e Fam. (2013) 29:354–6. doi: 10.32385/rpmgf.v29i6.11194
CrossRef Full Text | Google Scholar
38. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. (2001) 56:M146–56. doi: 10.1093/gerona/56.3.m146
PubMed Abstract | CrossRef Full Text | Google Scholar
39. Lohman M, Dumenci L, Mezuk B. Depression and frailty in late life: evidence for a common vulnerability. Journals Gerontol Ser B Psychol Sci Soc Sci. (2016) 71:630–40. doi: 10.1093/geronb/gbu180
CrossRef Full Text | Google Scholar
41. Martins J, Marques A, Teixeira PJ, Mota J, Lopes C, Nicola PJ. Socio-demographic factors associated with physical activity and sitting time patterns in adults: An analysis based on the Portuguese Food, Nutrition and Physical Activity Survey. Eur J Sport Sci. (2021) 21(2):250–60. doi: 10.1080/17461391.2020.1736643
PubMed Abstract | CrossRef Full Text | Google Scholar
42. Lopes C, Torres D, Oliveira A, Severo M, Guiomar S, Alarcão V, et al. National food, nutrition, and physical activity survey of the Portuguese general population (2015–2016): protocol for design and development. JMIR Res Protoc. (2018) 7:1–12. doi: 10.2196/resprot.8990
CrossRef Full Text | Google Scholar
43. Nikolić M, Milešević J, Zeković M, Gurinović M, Glibetić M. The development and validation of food atlas for portion size estimation in the Balkan region. Front Nutr. (2018) 5:1–8. doi: 10.3389/fnut.2018.00078
CrossRef Full Text | Google Scholar
44. Madeira T, Peixoto-Plácido C, Sousa-Santos N, Santos O, Alarcão V, Goulão B, et al. Malnutrition among older adults living in Portuguese nursing homes: the PEN-3S study. Public Health Nutr. (2018) 22(3):1–12. doi: 10.1017/S1368980018002318
PubMed Abstract | CrossRef Full Text | Google Scholar
45. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. (1987) 40:373–83. doi: 10.1016/0021-9681(87)90171-8
PubMed Abstract | CrossRef Full Text | Google Scholar
46. Lohman TJG, Roache AF, Martorell R, Roche AF, Martorell R. Anthropometric standardization reference manual. Chicago: Human Kinetics Books (1992):1–90. doi: 10.1249/00005768-199208000-00020
PubMed Abstract | CrossRef Full Text | Google Scholar
47. Ispoglou T, White H, Preston T, McElhone S, McKenna J, Hind K. Double-blind, placebo-controlled pilot trial of L-leucine-enriched amino-acid mixtures on body composition and physical performance in men and women aged 65–75 years. Eur J Clin Nutr. (2016) 70:182–8. doi: 10.1038/ejcn.2015.91
PubMed Abstract | CrossRef Full Text | Google Scholar
48. Negro M, Perna S, Spadaccini D, Castelli L, Calanni L, Barbero M, et al. Effects of 12 weeks of essential amino acids (EAA)-based multi-ingredient nutritional supplementation on muscle mass, muscle strength, muscle power and fatigue in healthy elderly subjects: a randomized controlled double-blind study. J Nutr Heal Aging. (2019) 23:414–24. doi: 10.1007/s12603-019-1163-4
CrossRef Full Text | Google Scholar
49. Koo GH, Woo J, Kang S, Shin KO. Effects of supplementation with BCAA and L-glutamine on blood fatigue factors and cytokines in juvenile athletes submitted to maximal intensity rowing performance. J Phys Ther Sci. (2014) 26:1241–6. doi: 10.1589/jpts.26.1241
PubMed Abstract | CrossRef Full Text | Google Scholar
50. Nelson ME, Rejeski WJ, Blair SN, Duncan PW, Judge JO, King AC, et al. Physical activity and public health in older adults: recommendation from the American college of sports medicine and the American heart association. Med Sci Sports Exerc. (2007) 39:1435–45. doi: 10.1249/mss.0b013e3180616aa2
PubMed Abstract | CrossRef Full Text | Google Scholar
51. Colado JC, Furtado GE, Teixeira AM, Flandez J, Naclerio F. Concurrent and construct validation of a new scale for rating perceived exertion during elastic resistance training in the elderly. J Sport Sci Med. (2020) 19:175–86. doi: 10.1249/mss.0b013e3180616aa2
CrossRef Full Text | Google Scholar
52. Guderian B, Johnson A, Mathiowetz V. Impact of exercise frequency on hand strength of the elderly. Phys Occup Ther Geriatr. (2013) 31:268–79. doi: 10.3109/02703181.2013.796583
CrossRef Full Text | Google Scholar
53. Sakugawa RL, Moura BM, da Orssatto LBR, de Bezerra ES, Cadore EL, Diefenthaeler F. Effects of resistance training, detraining, and retraining on strength and functional capacity in elderly. Aging Clin Exp Res. (2019) 31:31–9. doi: 10.1007/s40520-018-0970-5
PubMed Abstract | CrossRef Full Text | Google Scholar
54. Howatson G, Hoad M, Goodall S, Tallent J, Bell PG, French DN. Exercise-induced muscle damage is reduced in resistance-trained males by branched chain amino acids: a randomized, double-blind, placebo controlled study. J Int Soc Sports Nutr. (2012) 9:1–7. doi: 10.1186/1550-2783-9-20
PubMed Abstract | CrossRef Full Text | Google Scholar
55. Zurauskaite G, Meier M, Voegeli A, Koch D, Haubitz S, Kutz A, et al. Biological pathways underlying the association of red cell distribution width and adverse clinical outcome: results of a prospective cohort study. PLoS One. (2018) 13:1–13. doi: 10.1371/journal.pone.0191280
CrossRef Full Text | Google Scholar
56. Martínez-Velilla N, Ramírez-Vélez R, De Asteasu ML S, Zambom-Ferraresi F, Garciá-Hermoso A, Marín-Epelde I, et al. Red blood cell distribution width trajectory during a multicomponent exercise in hospitalized older adults: a secondary analysis of a randomized clinical trial. Rejuvenation Res. (2021) 24:294–6. doi: 10.1089/rej.2020.2405
CrossRef Full Text | Google Scholar
57. Hoogendijk EO, Flores Ruano T, Martínez-Reig M, López-Utiel M, Lozoya-Moreno S, Dent E, et al. Socioeconomic position and malnutrition among older adults: results from the fradea study. J Nutr Heal Aging. (2018) 22:1086–91. doi: 10.1007/s12603-018-1061-1
CrossRef Full Text | Google Scholar
58. Lochlainn MN, Cox NJ, Wilson T, Hayhoe RPG, Ramsay SE, Granic A, et al. Nutrition and frailty: opportunities for prevention and treatment. Nutrients. (2021) 13:1–20. doi: 10.3390/nu13072349
CrossRef Full Text | Google Scholar
60. Aoyama K, Tsuchiya M, Mori K, Kubo Y, Shiraishi K, Sakaguchi E, et al. Effect of a late evening snack on outpatients with liver cirrhosis. Hepatol Res. (2007) 37:608–14. doi: 10.1111/j.1872-034X.2007.00036.x
PubMed Abstract | CrossRef Full Text | Google Scholar
61. Hernández-Conde M, Llop E, Gómez-Pimpollo L, Fernández Carrillo C, Rodríguez L, Van Den Brule E, et al. Adding branched-chain amino acids to an enhanced standard-of-care treatment improves muscle mass of cirrhotic patients with sarcopenia: a placebo-controlled trial. Am J Gastroenterol. (2021) 116:2241–9. doi: 10.14309/ajg.0000000000001301
CrossRef Full Text | Google Scholar
62. Siramolpiwat S, Limthanetkul N, Pornthisarn B, Vilaichone RK, Chonprasertsuk S, Bhanthumkomol P, et al. Branched-chain amino acids supplementation improves liver frailty index in frail compensated cirrhotic patients: a randomized controlled trial. BMC Gastroenterol. (2023) 23:1–10. doi: 10.1186/s12876-023-02789-1
PubMed Abstract | CrossRef Full Text | Google Scholar
63. Zhang Z, Gao S, Dong M, Luo J, Xu C, Wen W, et al. Relationship between red blood cell indices (MCV, MCH, and MCHC) and major adverse cardiovascular events in anemic and nonanemic patients with acute coronary syndrome. Dis Markers. (2022) 2022:1–12. doi: 10.1155/2022/2193343
CrossRef Full Text | Google Scholar
64. Cecchi F, Pancani S, Vannetti F, Boni R, Castagnoli C, Paperini A, et al. Hemoglobin concentration is associated with self-reported disability and reduced physical performance in a community dwelling population of nonagenarians: the mugello study. Intern Emerg Med. (2017) 12:1167–73. doi: 10.1007/s11739-017-1762-1
PubMed Abstract | CrossRef Full Text | Google Scholar
65. Hu M, Finni T, Sedliak M, Zhou W, Alen M, Cheng S. Seasonal variation of red blood cell variables in physically inactive men: effects of strength training. Int J Sports Med. (2008) 29:564–8. doi: 10.1055/s-2007-989320
PubMed Abstract | CrossRef Full Text | Google Scholar
66. Kristal-Boneh E, Froom P, Harari G, Shapiro Y, Green MS. Seasonal changes in red blood cell parameters. Br J Haematol. (1993) 85:603–7. doi: 10.1111/j.1365-2141.1993.tb03354.x
PubMed Abstract | CrossRef Full Text | Google Scholar
67. Schumacher YO, Jankovits R, Bültermann D, Schmid A, Berg A. Hematological indices in elite cyclists. Scand J Med Sci Sports. (2002) 12:301–8. doi: 10.1034/j.1600-0838.2002.10112.x
PubMed Abstract | CrossRef Full Text | Google Scholar
68. Boiko ER, Bashkanov AS, Maklakova GN, Potolitsyna NN. Human peripheral blood parameters under conditions of low temperatures of the far north. Hum Physiol. (2001) 27:127–8. doi: 10.1023/A:1007179929279
CrossRef Full Text | Google Scholar
70. Lee JH, Suh Y, Park J, Kim GU, Lee S. Combined effects of handgrip strength and sensory impairment on the prevalence of cognitive impairment among older adults in Korea. Sci Rep. (2022) 12:1–9. doi: 10.1038/s41598-022-10635-9
PubMed Abstract | CrossRef Full Text | Google Scholar
71. Kornilov SA, Zhukova MA, Ovchinnikova I V, Golovanova I V, Naumova OY, Logvinenko TI, et al. Language outcomes in adults with a history of institutionalization: behavioral and neurophysiological characterization. Sci Rep. (2019) 9:1–13. doi: 10.1038/s41598-019-40007-9
PubMed Abstract | CrossRef Full Text | Google Scholar
72. Dayanand K, Olivia E., Atherton , Jennifer L. Tackett2, emilio Ferrer1 and RWR. 乳鼠心肌提取 HHS public access. Physiol Behav (2018) 176:139–48. doi: 10.1002/wsbm.1219.Branched
CrossRef Full Text | Google Scholar
73. Verlaan S, Aspray TJ, Bauer JM, Cederholm T, Hemsworth J, Hill TR, et al. Nutritional status, body composition, and quality of life in community-dwelling sarcopenic and non-sarcopenic older adults: a case-control study. Clin Nutr. (2017) 36:267–74. doi: 10.1016/j.clnu.2015.11.013
PubMed Abstract | CrossRef Full Text | Google Scholar
74. Drageset J, Eide GE, Nygaard HA, Bondevik M, Nortvedt MW, Natvig GK. The impact of social support and sense of coherence on health-related quality of life among nursing home residents–a questionnaire survey in Bergen, Norway. Int J Nurs Stud. (2009) 46:65–75. doi: 10.1016/j.ijnurstu.2008.07.005
PubMed Abstract | CrossRef Full Text | Google Scholar
75. Coelho-Junior HJ, Marzetti E, Picca A, Cesari M, Uchida MC, Calvani R. Protein intake and frailty: a matter of quantity, quality, and timing. Nutrients. (2020) 12(10):2915. doi: 10.3390/nu12102915
PubMed Abstract | CrossRef Full Text | Google Scholar
76. Roh E, Choi KM. Health consequences of sarcopenic obesity: a narrative review. Front Endocrinol. (2020) 11:1–12. doi: 10.3389/fendo.2020.00332
CrossRef Full Text | Google Scholar
77. Han CY, Miller M, Yaxley A, Baldwin C, Woodman R, Sharma Y. Effectiveness of combined exercise and nutrition interventions in prefrail or frail older hospitalised patients: a systematic review and meta-analysis. BMJ Open. (2020) 10:1–13. doi: 10.1136/bmjopen-2020-040146
CrossRef Full Text | Google Scholar
78. Furtado GEGE, Carvalho HM, Loureiro M, Patrício M, Uba-Chupel M, Colado JCJC, et al. Chair-based exercise programs in institutionalized older women: salivary steroid hormones, disabilities and frailty changes. Exp Gerontol. (2020) 130:1–11. doi: 10.1016/j.exger.2019.110790
CrossRef Full Text | Google Scholar
link







