
Incidence and predictors of pregnancy among reproductive-age women in an ART clinic of public health facilities in Arsi zone, southeastern ethiopia: a five-year retrospective cohort study | BMC Women’s Health

Study design and period
An institution-based retrospective cohort study design was employed, utilizing client logbook from ART clinics in selected public health institutions in the Arsi Zone of central Ethiopia, from December 1, 2013, to April 30, 2019.
Study area
A continuous follow-up of client records at selected public hospitals and health centers in the Arsi zone and Asella administrative town was used to conduct the study. Arsi zone is located 175 km southeast of Addis Ababa and is divided into 27 Woredas and two administrative towns namely Bokoji Town and Asella Town. Asella is the town also serving the zone as a capital. The Arsi zone and Asella town have one teaching referral hospital in common, six district hospitals, 102 functional health centers, and 498 health posts which currently provide the health service for the population. ART service has been provided by 32 health centers and seven hospitals during the study period based on the WHO guideline [38]. Most of the institutions began within the last five years of the study period providing ART including all the district hospitals through the path meandering to attain the stated number. The total population of Arsi Zone as projected from the 2007 census is estimated at 3.5 million.
The total ART service users during the study period in the Arsi zone including Asella Town was 8514. Proportion revealed female 4919 (57.78%), male 2942 (34.55%), and children less than 15 years 653 (7.67%). The number of PLWHA on ART during the study period in Asella Teaching Referral Hospital and Asella Health Center is somewhat larger than half the total number in multiple health facilities in Arsi Zone, 4371 (51.34%). The source of information was the Arsi Zone Health Department ART service database.
Source population and study population
All women on ART in Hospitals and Health Centers of Arsi Zone and Asella Administrative town were the source population for this study. All women who were on antiretroviral treatment and registered for follow-up care from December 2013 to April 2019 in the selected hospitals and health centers were taken as the study population for this study.
Inclusion and exclusion criteria
Records of sexually active, reproductive-age women receiving antiretroviral therapy at the facility between December 2013 and April 2019 were included in the study. However, the study excluded records of mothers who had more than one pregnancy during the follow-up period in the hospital, as well as those of women receiving pre-ART treatment, who began ART based on option B+.
Sample size determination and procedure
The sample size for the study was calculated using a formula for the estimation of single population proportion. In a previous study in Ethiopia [5] there was 10.976% of pregnancy incidence. Considering a 95% confidence level and 3% margin of error, sample size determined: initial sample size (n) = z2p(1-p)/d2 = (1.96)2 0.10976(1-0.10976)/0.03 × 0.03 = 417 women. Adding 20% to compensate for incomplete records, the final sample size was determined to be 500.
The study included six health facilities that began providing ART services in 2012 to ensure the inclusion of clients who started treatment in the past five years (December 2013 to April 2019), increasing the likelihood of capturing relevant cases. While 32 health centers and seven hospitals offered ART services during the study period in the study area, only 10 facilities were operational a decade ago. Facilities with shorter service durations were excluded to avoid skewing risk assessments. The selected facilities; Asella Hospital, Abomsa Hospital, Robe Hospital, Bokoji Health Center, Huruta Health Center, and Asella Health Center were chosen based on their service duration. Systematic random sampling was applied based on the average monthly client load to select records at each facility, with data collection continuing until the required sample size was reached (Fig. 1).
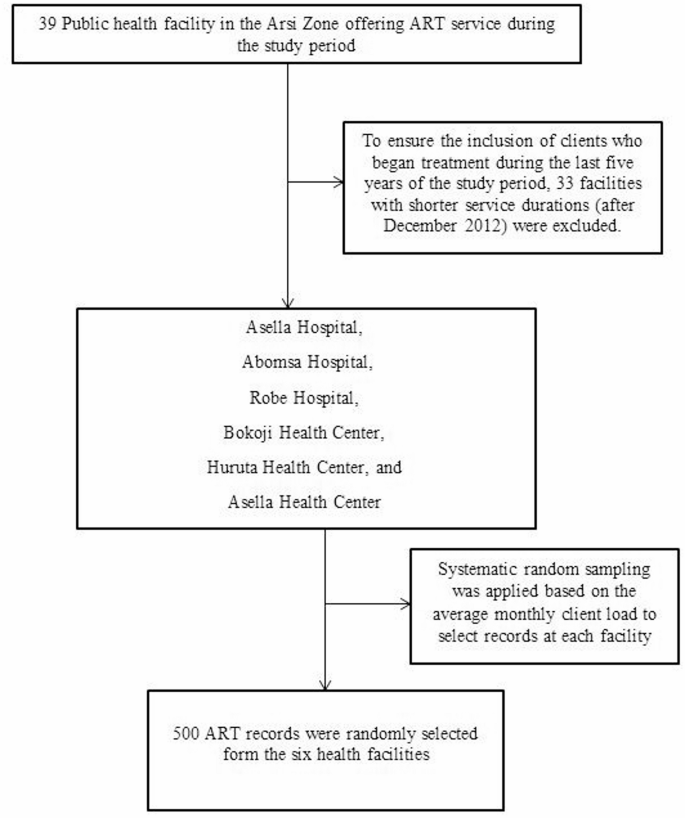
Diagrammatic representation of the study sampling procedure
Variables of the study
Dependent
The study measures the incidence of pregnancy which was labeled as yes or no., and the trends of fertility across five years.
Independent
It identifies the positive as well as negative determinants of fertility and outcome for the study population in a specific that includes socio-demographic characteristics such as age, residence, marital status, occupation, educational status, number of children, and clinical characteristics like CD4 count, WHO staging [38], weight, BMI, and functional status of women on ART, follow-up behaviors as regular or irregular.
Operational definitions
Pregnancy: is clinically confirmed and documented by the health service provider. Incidence of Pregnancy: This is considered the first pregnancy after ART enrollment within the follow-up time. Time to Event: In this research, time to event is defined as the time from enrollment on ART to the conception of the first pregnancy. The exposure was considered positive for those who were in a reproductive age group and who were on ART during the time in the study period.
Data collection tools and procedures
A structured data collection checklist in English was used to extract data from the records. Data were extracted from the records of the selected health institutions. ART intake forms and cards were used to extract information that was not available in the main logbooks. The data were collected by health information specialists of the institutions working on the ART database and supervised by two public health professionals. The investigators had weekly checkups of the filled forms.
Data quality control
Training of two days was given for the data collectors and the supervisors before the actual data collection. Completeness of data was checked in each day of activity and the necessary feedback was offered to data collectors the next morning. Besides this, the principal investigators and an experienced data clerk carefully enter and thoroughly cleaned the data before the commencement of the analysis. Since we were using secondary data, the study’s main drawback is the missing data. To enhance the study’s quality, we have taken into account the incomplete and missing records as a non-response rate.
Data management and analysis
Data extracted from the record set were entered into formatted EPI Info version 7.0 and exported to Stata 14 for analysis. Descriptive statistics and incidence rate of pregnancy in person-years of follow-up were reported. A Kaplan-Meier curve with hazard and survival functions was used to estimate the probability of becoming pregnant. The Cox proportional hazards model was used and results were expressed as hazard ratios with 95% CIs. Variables with p-value ≤ 0.25 at Kaplan-Meier survival analysis were entered into the multivariable Cox proportional hazards model to identify the independent predictors of pregnancy. An adjusted hazard ratio with 95% CI was used to report the findings.
link




